
Cancer and Barrett's esophagus
Written by:Is Barrett's esophagus related to cancer?
Gastroesophageal reflux, in addition to causing discomfort, such as a burning or burning sensation in the area of the sternum or throat, reflux of food material into the mouth, pain in the upper abdomen, precordial pain - similar to that of angina, lack of appetite or feeling of satiety after the intake of small amounts of food, is also linked to the so-called Barrett's Esophagus. Because of this, all gastroesophageal reflux, either acidic or weakly acidic, must be well controlled by endoscopy and correctly diagnosed and treated with diet, antireflux intervention or medication, in order to reduce the risk of progression to Barrett's esophagus, and subsequently to adenocarcinoma.
It is essential to make clear the concept that reflux has to be well treated and diagnosed by a specialist. Proton pump inhibitors are of little use in an alkaline reflux, with biliary or weakly acidic material, since they contribute to their alkalinization. Therefore, esophageal pHmeth- estry with detection of acid and alkaline reflux should be mandatory.
Thus, the American College of Gastroenterology (ACG) has come to a series of conclusions on this.
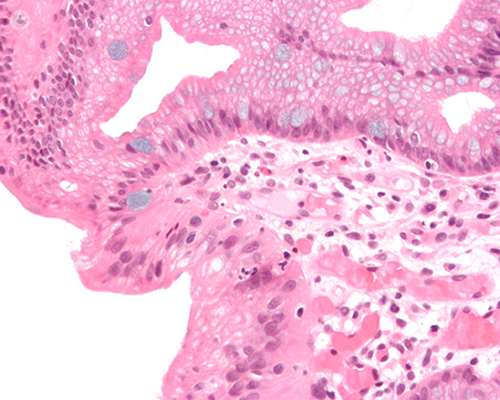
Barrett's esophagus: the study
In patients with Barrett's esophagus, low-grade dysplasia carries a considerable risk for the progression of esophageal adenocarcinoma, the risk of progression in these patients being eight times greater than in patients diagnosed without dysplasia.
And, in the words of Dr.. Krishnamoorthi, of the ACG, "subjects with Barret's esophagus diagnosed with low-grade dysplasia may be candidates for endoscopic therapy. Endoscopic ablation is a recommended strategy for these patients, "he said.
Thus, we evaluated whether a diagnosis of low-grade dysplasia is associated with the risk of progression. To do this, a retrospective study was used in which data from almost two thousand (1998) patients with a long Barret segment in their esophagus and almost one thousand (952) with esophageal adenocarcinoma were reviewed.
Gastrointestinal pathologists reviewed demographics, histological data, endoscopic findings, and low-grade dysplasia index biopsy samples. After diagnosis, patients were grouped into five groups: low-grade dysplasia, high-grade dysplasia, adenocarcinoma, indefinite dysplasia, or without Barret's esophagus dysplasia. Thus, in the final sample, 249 patients with a diagnosis of low-grade dysplasia were collected, among which were 201 men and 48 women, with a mean age of 64.3 years.
We then identified patients whose disease progressed from low grade dysplasia to high grade dysplasia or adenocarcinoma.
Barrett's esophagus: progression of dysplasia from low to adenocarcinoma
During a mean follow-up of almost eight years, fifteen patients progressed to high-grade dysplasia or adenocarcinoma. The time to progression was lower in the low grade group of confirmed dysplasia and in the indefinite group of dysplasia than in the group without dysplasia, once adjusted for age, smoking, sex, Barrett segment length and other characteristics of the disease.

