
El pronóstico de los meningiomas es muy bueno si la extirpación del tumor es total
Written by:Meningioma is a normally benign, slow-growing tumor that originates in one of the roofs (arachnoids) of the Central Nervous System. Most of the time, it is usually well circumscribed and encapsulated, allowing it to be perfectly separated from adjacent nerve tissue. It may be located in the intracranial cavity and also in the intrarectal cavity, although in the latter in a lower proportion.
Incidence of meningioma
It is a relatively frequent tumor, appearing in 3% autopsies (for whatever reason) in people over 60 years. Within the skull its frequency ranges from 14% to 19% of primary intracranial tumors. It is more frequent in women than in men in a ratio of 1: 8: 1 and its highest incidence is at 45 years of age.
What types of meningioma are there?
By their nature, most are benign, as previously stated, but there is a relatively low percentage of meningiomas that have abnormal behavior, showing some aggressiveness, even with infiltration of brain tissue. Within the latter are those classified as atypical, rhabdoid or malignant.
The most frequent location of these tumors in descending order is: parasagittal (attached to the wall of the superior longitudinal sinus which is a collecting vein of both cerebral hemispheres and is large), convexity of the hemispheres, tubercle selar (very close to the pituitary gland), the sphenoid wing (middle cranial fossa), the olfactory groove (anterior cranial fossa base), and the sickle of the brain (a structure that separates both cerebral hemispheres).
Causes of meningiomas
The occurrence of meningiomas has been related to previous exposure of the patient to ionizing radiation both at high doses and at low doses, for whatever reason.
Since women are twice as likely as men to develop meningiomas, and these tumors also have hormone receptors, the hormone factor (exogenous and endogenous) has been considered as a possible triggering factor.
There is nothing that can prevent the onset of a meningioma.
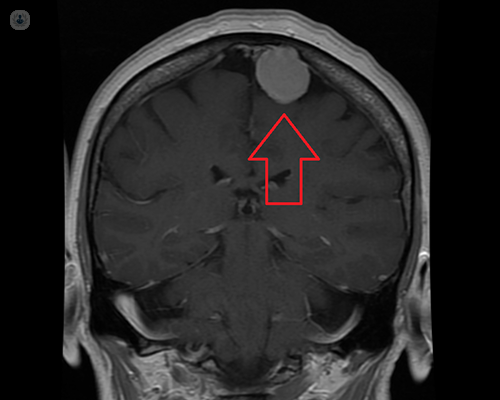
Diagnosis of meningiomas
Computed tomography (CT) is the most commonly used test in the emergency department of hospitals to diagnose the presence of a meningioma. Once this is done, the next step will be the realization of a nuclear magnetic resonance (NMR) that will give us not only much more information as to the characteristics and nature of the tumor, but also as to the location, relation of adjacent anatomical structures and possible involvement of cerebral arteries and veins.
If we want to know more about the involvement of these vascular structures mentioned, we will use as a first approximation to what is called an angio-MRI, and if we still want to have more detail of this circumstance we would have to proceed to the practice of cerebral angiography. Generally, this is an invasive test that requires puncture of the femoral artery and the introduction of a catheter that is directed through the aorta artery to the cerebral arteries, both carotid and vertebral.
Prognosis of meningiomas
The prognosis is very good if the removal of the tumor is complete, and here we must include the base of implantation in the dura mater, as well as the bone involvement, if there was. The problem is that sometimes the tumor can not be completely resected by having arteries or veins inside it that can not be sacrificed due to its involvement in eloquent areas of the brain. Obviously, its interruption would lead to serious sequelae. In case this happens, it is preferable to either leave a tumor rest without extirpation and see the evolution thereof over time, or treat it with radiotherapy in one or several fractional doses.
Treatment of meningiomas
Surgery is the treatment of choice for symptomatic meningiomas. Meningiomas that we may encounter incidentally and that do not have edema in the MRI or those that present only epileptic seizures controlled with medication can be managed in a conservative way, besides being controlled periodically with imaging techniques with the aim of preventing tumor growth in the future.
Since meningiomas are usually a highly vascularized tumor, the surgical technique will be to interrupt the arteries being irrigated as soon as possible. Then a removal of the tumor inside its capsule will be done to gain space and not have to displace the adjoining brain structures. The capsule will then be dissected, which can be folded gradually thanks to the internal decompression we have carried out. Once the tumor is completely resected, if possible, removal of the dura and affected bone will proceed.
For more information, consult your neurosurgery specialist .

