How cavities and plaque form
Written by:To understand the pathology cariogenic have to go back to our origins because from the beginning several evolutionary types have developed different ways to grow under the Earth 's gravity. Some living beings evolved in the water and did not require rigid structures to keep the volume of your body against gravity, for example jellyfish. Others used protein elements such as cartilage (fish), keratin (exoskeleton turtles), cellulose (plant), and other most evolved form a hard skeleton based on calcium salts to support and maintain your body under the weight of the gravity. Among the latter, on the one hand we would find exoskeletons formed by minerals of calcium carbonates (coral), and secondly those using other mineral much more complex as hydroxyapatite to form their endoskeleton as in the case of mammals.
We as mammals, have a scaffold of hydroxyapatite in the form of hexagonal crystals, which are our ladrillitos to form the "endo skeleton and teeth". This ladrillito is soluble in acid, but much less than the calcium salts of carbonates above. That is, our teeth are much more resistant to acid attack.
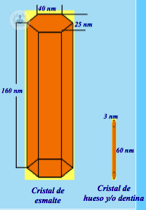
Ladrillito or calcium hydroxyapatite crystallite. The large hexagonal crystallite is enamel, dentin small and bone.
The teeth are formed inside our bones excretory cells by a protein matrix that induces its calcium crystallization (our ladrillitos hydroxyapatite), generating the enamel covering the external crown. This glaze is a-cell and initially their hydroxyapatite crystallites are small (immature enamel) but eventually expand becoming very large, tough and poorly soluble acid (mature enamel) with 94% calcium. Coated enamel dentin if cell with 60% calcium and the remainder are the cells and water; At its center is the dental pulp with life-support vessels, nerves sensitivity / pain and the cell bodies of the dentin.
Specifically, the enamel is formed by crystallites of hydroxyapatite (94%) spatially arranged such that under observed as tufts in the inner part microscope, called "enamel prisms or prismatic enamel", and as if it were a compact lawn called "aprismatic enamel" in the superficial or external face and the internal interface with the dentine.
Each tooth has a shape and a very specific spatial position to properly carry out its function. If the masticatory function is physiological, the food itself when cut or crushed clean the tooth surface friction (self-cleansing), still remains swallowing. In addition, it also has the saliva, wetting agent and cleaner drags, leaving the tooth surface a film adhered protective effect known as "acquired film" which if not constantly renews it was transformed into the famous "plaque" the added bacteria and food debris.

Orthopantomography with mixed dentition.
With this introduction, to understand how the "Cavities" is formed is now easier. The consolidated with food debris, plaque releases acids during decomposition, producing enamel surface solutions. Said enamel need an acidic pH below 5.5 to dissolve, being the normal pH of a healthy mouth of 7.4 (an alkaline base). This pH is controlled by the "saliva" by a "buffer" (bicarbonates and phosphates), ie, the ability to neutralize pH variations which occur when eating system.
When we eat any food, the pH drops a full point, or 7.4 to 6.4, and it takes about one hour to neutralize. But what happens if you ever eat before the end of that time ?, Then the pH back down another point from the pH had plenty. If this was in 6.8, he would drop to pH 5.8 if everything was correct, but if the patient did not have a proper buffer system would need more than 2 hours to recover the initial pH, and therefore, it would be easier to reach a pH below 5.5, producing many areas of dissolution and leaving cavitations or hollows where Palca accumulates, colonizándose with multifarious bacteria etc.

Photo of a Fantomas where the most frequent onset of decay, interproximal and occlusal pits face is observed
Among the multifarious bacteria, we have cataloged as "cariogenic", mainly represented by various types of "streptococcus, lactobacillus acidophilus, Actinomyces viscosus" among others, as they secrete acids and proteolytic enzymes that dissolve the enamel and proteins in successive stages dentin, creating cavities and clinically detectable. Therefore the injury initiated by the acids are perpetuated by cariogenic bacteria becoming a DECAY. If no bacteria will be no decay.
On the other hand, we must also take into account the protective capacity of saliva. It adheres to the enamel and exposed roots of the teeth forming an insoluble film thanks to its glycoproteins that make up the famous "acquired film". If the film is successful, it protects teeth against acid, but in turn also helps bacteria from adhering, thus initiating the known "plaque" when it is not renewed properly by the self - cleansing or daily oral hygiene.
"The initial dental plaque" progresses as is being incorporated food remains and new bacteria, thus forming a "biological film" where bacteria and secrete polysaccharides long chains that help increase adhesion and firmness of the same tooth. This process is enhanced by the sugars incorporated mouth feeding and biofilm bacteria becoming more acidic (low pH), "cariogenic infection is established". Over time, if the plaque is removed no complexity will increase and not only is colonized by many bacteria types, but also by "viruses, fungi, protozoa, etc.". If a dental plate permanently resides in that area, calcification which initially is fragile-white and dark later known as the "dental plaque" it will start. With the presence of plaque pathology known as gingivitis can progress to paradontopatías start.