
¿Por qué me cuesta tragar?
Written by:Dysphagia is difficulty swallowing. It is a very common problem that is present in many diseases; It can also cause life-threatening problems such as aspiration pneumonias.
Diagnosis of dysphagia
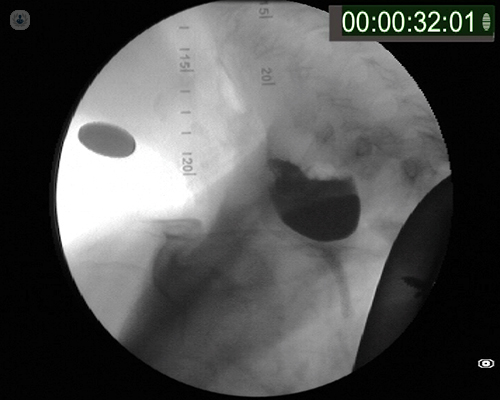
The diagnosis of dysphagia is based on several tests, some of them clinical, others endoscopic (such as swallowing Videoendoscopy) and other functional or radiological tests (such as videofluoroscopy). The etiopathogenic diagnosis that can be obtained with these tests is key to propose a suitable treatment.
Treatment of dysphagia
The treatment of dysphagia is fundamentally dietary and rehabilitative, although sometimes we can perform more invasive procedures that seek to improve the efficiency of swallowing, such as the treatment of certain sphincters or the improvement of closure of the glottis; a thyroplasty in case of laryngeal paralysis or exceptional measures aimed at avoiding the possible aspirations (through a laryngeal exclusion or separation of the airway from the digestive tract). Other procedures treat specific processes, such as a Zenker diverticulum. Finally, it may sometimes require a gastrostomy to facilitate prolonged enteral nutrition.
Some patients, especially with certain neurodegenerative disorders, may present an excessive tonic contraction of the cricopharyngeal muscle, a fundamental component of the upper esophageal sphincter. This contraction, called the cricopharyngeal bar , can be treated by a procedure called cricopharyngeal myotomy, which can be performed by an external cervicotomy approach with a series of risks and possible complications, and which has traditionally been indicated in cases with marked increase in contracture said sphincter causing a closing of the passage of the alimentary bolus increasing the resistances to said passage.
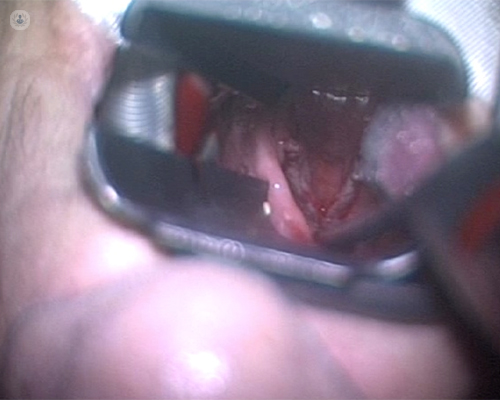
The old open surgery procedures have been replaced by endoscopic techniques with laser or mechanical instruments, and in certain cases, if the fibrotic origin of the cricopharyngeal closure is discarded, botulinum toxin type A can be infiltrated in the cricopharyngeal muscle, causing a blockage neuromuscular and a relaxation during a few months of this contracture and improving swallowing in cases in which the contracture is responsible for the swallowing alteration. Its effect is reversible and it may be necessary to repeat infiltrations.
Care must be taken in the location of the injection as it may spread to other muscle groups causing pharyngolaryngeal paralysis, which may aggravate the patient's condition.
Consequences of a sustained cricopharyngeal contracture
One consequence of a sustained cricopharyngeal contracture is the production of a diverticulum by herniation of the pharyngeal mucosa through the Lainert triangle, a fact that can form a bag where food accumulates.
The treatment of the diverticulum was carried out classically by the same approach of the myotomy, but at the moment other endoscopic techniques exist as they are the laser myotomy or with systems of autosutura mechanical, like those used in the abdominal surgery.
It is used in patients with a primary contracture of the cricopharynx, sometimes as a diagnostic and prognostic test before indicating a myotomy.
Sometimes there is an incompetence of the glottic sphincter, in vocal cords, either by paralysis or another neuromuscular alteration at that level; in these cases, in addition to the rehabilitation of phonation itself, may require mediatorial treatments of the glottis (which can be surgical, by means of the placement of a prosthesis) or techniques of infiltration of various substances (hydroxyapatite gel, collagen, autologous fat, etc.), which can be performed by endoscopic, transoral or percutaneous.
The result of the infiltration tends to be temporary, whereas the thyroplasty has a more permanent result. Occasionally, this is associated with an arytenoid adduction procedure that increases closure at the posterior glottic level.
Finally, in cases of failure of all treatments, airway exclusion techniques can be performed using laryngeal exclusion techniques, endoscopic closure of the supraglottis (currently in some centers can be performed by transoral robotic surgery) or, in last extreme, a total laryngectomy.
For more information consult with the otorhinolaryngologist .


