
Facial reconstruction with 3D technology
Written by:The evolution of technology and knowledge does not follow a linear path. Knowledge does not accumulate like sand on a beach, little by little; They are rather like storms, which appear abruptly and take away the old and put the new.
Thus, at the end of century XVIII the steam engine propitiated the first industrial revolution. At the end of the 19th century and the first years of the 20th century, electrification and the internal combustion engine were the starting point of the second industrial revolution. There are many indications that at the end of the 20th century a third industrial revolution began, this time based on computerization and robotization.
Between each revolution technical progress and improvements for humanity have been slowed down. During each industrial revolution the changes have been more dramatic and evident.
Similarly, surgical techniques advance at varying rates. There are decades where progress seems imperceptible, and one has to put some distance to see the improvement. In contrast, there are short periods of time in which it seems that the advance is much greater than in previous years.
The twentieth century gradually transformed surgical procedures, which were once dramatic, risky, often deadly, events that were almost always routine (blessed routine!), With increasingly predictable and less risky results. General anesthesia, endotracheal intubation, antisepsis, antibiotics, blood transfusions, advances in physiology and pharmacology, osteosynthesis, advances in anatomical knowledge, are some of the steps towards improving surgical procedures.
Reconstructive surgery of the maxillofacial area has undergone changes over time. In some times the changes were gradual. However, there have been years in which the pace of progress has accelerated. The most radical innovations. The results for the patients, extraordinarily better.
Mandibular reconstruction is one of the aspects where the technical advances of maxillofacial surgery are best appreciated: several milestones accompanied by a general refinement of the techniques.
In the 1960s and 1970s, mandibular reconstruction was based on the use of hip or rib bone grafts, with very poor results overall. These bone grafts were nourished by diffusion of the surrounding tissues. Something similar to the respiration of insects, which collect oxygen from the air directly through holes in their shell. It was a good idea for small amounts of tissue, but for large segments of bone in contact with the oral cavity, colonized by bacteria, a poor solution. It seemed better to use titanium plates and screws that bridged the defect and kept the rest of the jaw in position. But that did not work either: except in very specific cases, the screws would loosen and the plates would break or peek outward, breaking the skin or mucous membrane of the mouth.
In the 1970s and 1980s, the use of revascularized grafts was a revolution in mandibular reconstructive surgery: bone grafts are designed to conserve blood supply by reconnecting arteries and veins to blood vessels in the head and neck using a microscope surgical. The most commonly used graft is the fibula. The peroneal artery and vein are attached to blood vessels of the neck by points of sutures almost invisible to the naked eye. The fibula segments are joined to each other and to the rest of the jaw by means of plates and screws of osteosynthesis, which work phenomenally whenever there is bone. Thus, from the outset the graft is a vascularized structure that does not become infected and which heals normally, as if it were a standard bone fracture fixed with plates and screws.

During the following years these techniques have been refined with "minor" improvements: greater experience and skill of surgical teams, better postoperative management of patients, use (never systematic) of dental implants to allow more normal chewing to patients, etc.. Dental implants were not commonly put on these patients because the position of the new bone was often very unsuitable for connecting dental prostheses.
At the beginning of the 21st century, an important obstacle still remained: in mandibular reconstruction with vascularized bone, the size and angulations of the graft, as well as the final orientation of the graft in the mandible, were decided "by eye", making measurements with a ruler to make That the new jaw seems as normal as possible. It was an impossible task: the lack of precision inherent in this method meant that patients were left with alterations in dental occlusion (the remaining upper and lower teeth did not fit together), and the mandibular contour always remained to some degree Of deformation.

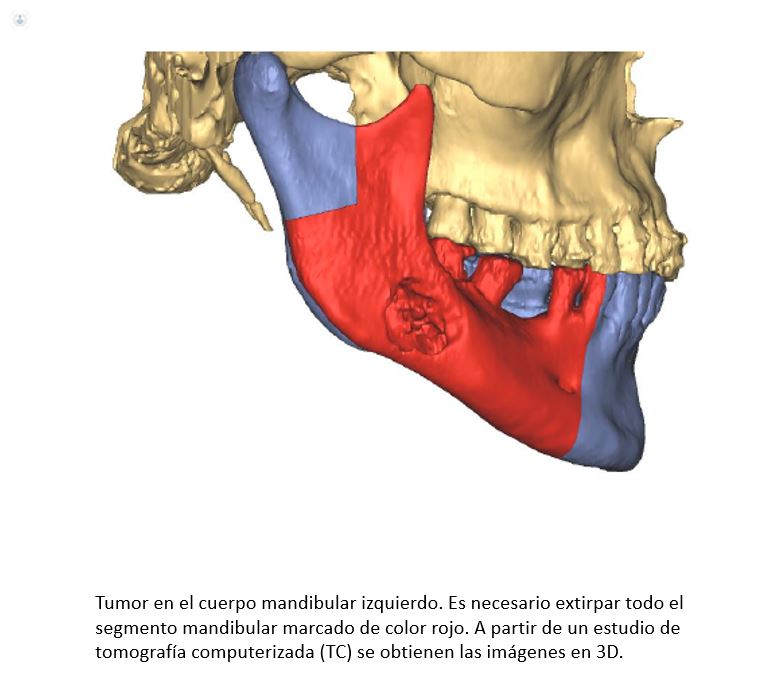
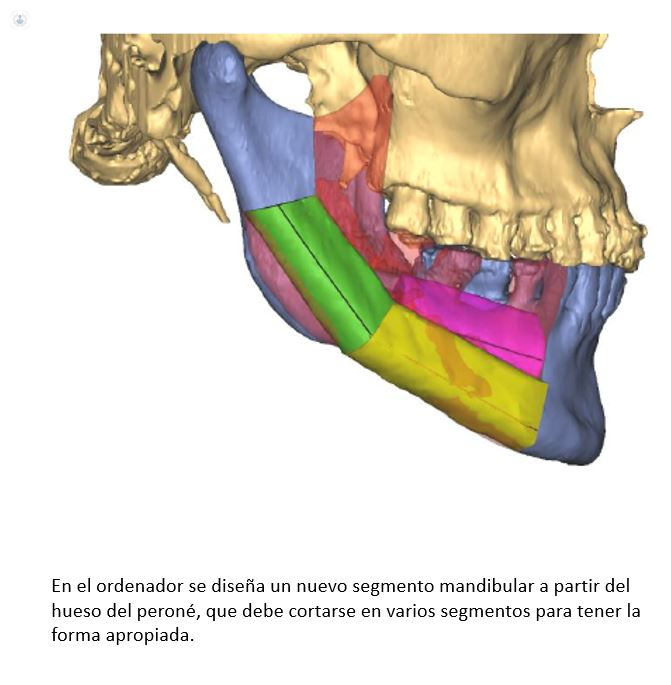
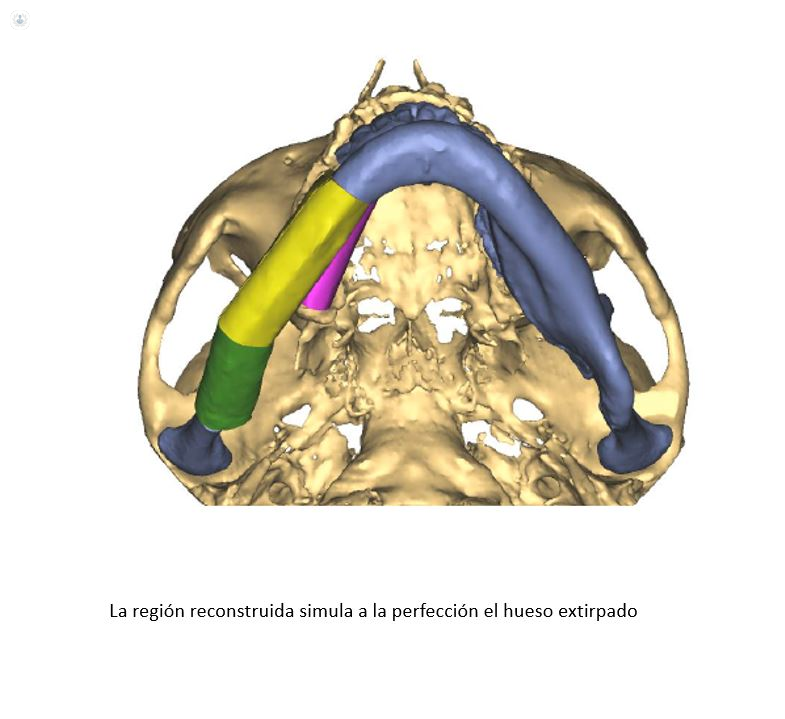
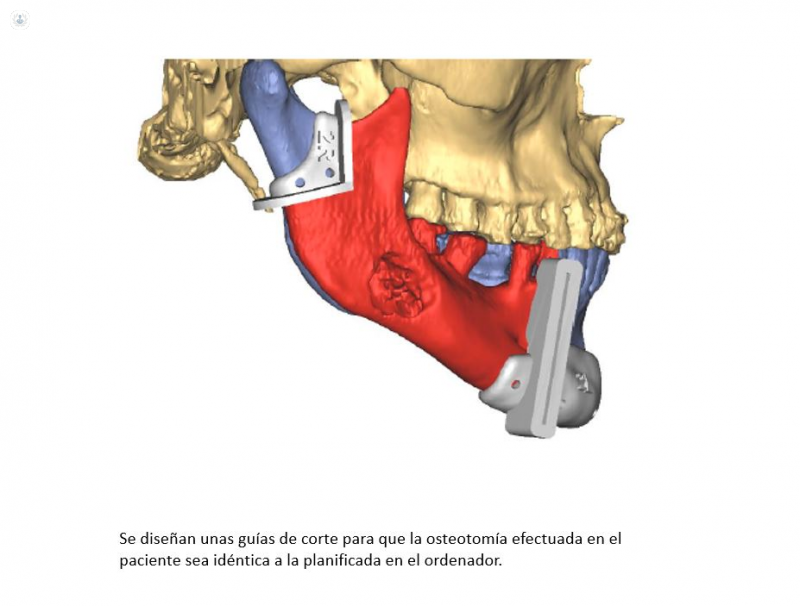
That is when the revolution occurs. And it is a revolution linked to the third industrial revolution, that of computer science: three-dimensional medical imaging techniques give us a very precise picture of the shape of the tissues in which we work. By using the computer for the three-dimensional simulation of the mandible and fibula, the position, angulation and placement of each of the bone segments can be designed with great precision, in addition to designing before the intervention an osteosynthesis plate that adapts Exactly to the bony contours.
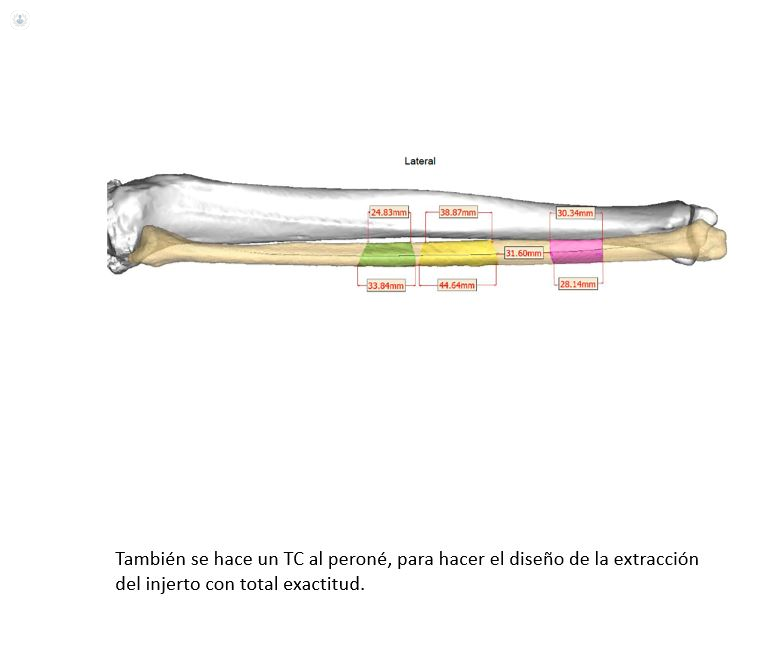
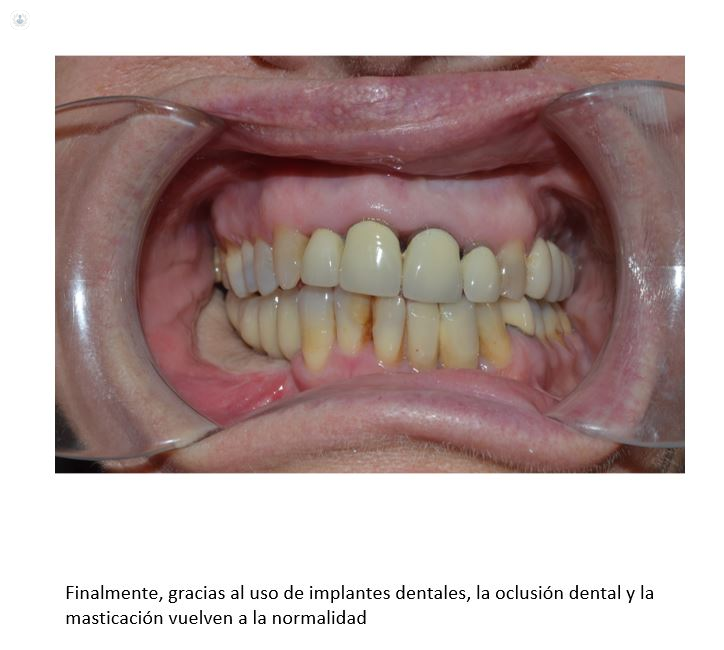
Thanks to 3D printing techniques, all that virtual work on the computer can be translated into the real world as stereolithographic models of the jaw, the fibula, and as cutting guides that indicate with unprecedented accuracy the location and angulation of osteotomies. The surgical procedure is much more precise and simple, the surgical time is reduced in several hours, and the result is a mandible with preserved dental occlusion, and symmetrical and natural mandibular contours. In recent years we have used this technology to perform mandibular reconstructions with an accuracy impossible to achieve with traditional methods.

The road has been long: in the 60's, patients who lost the mandibular bone due to trauma or tumor resection had to coexist with a deformity so invalidating that many did not leave their homes the rest of their life. Now we are getting something extraordinary: that patients return to live a normal life ... an "ordinary". Entering and leaving home, going to the movies, going to a restaurant. Only people who have ever seen such seemingly simple life activities limited their understanding of the advancement this entails.

