How to treat different types of brain and intracranial tumors
Written by:Neurooncology is the branch of medicine that treats tumors of the nervous system: brain, spinal cord and peripheral nerves.
It is important to keep in mind that in the treatment of these tumors, although the neurosurgeon plays a major role, there are and must be more specialists involved, such as radiologists, pathologists, medical oncologists and radiologists (among others). Multidisciplinary approach and, therefore, more effective of the problem.
It is also very necessary to have a clear concept: the most important part of the brain is its function, and the most important thing for the individual is its brain, so whenever an injury is treated that can affect brain functionality, And the benefits of more or less radical surgery, as well as the possibility of using less aggressive treatments in certain types of tumors, such as some neurinomas and meningiomas.
Brain and Intracranial Tumors
Cerebral and intracranial tumors are, fortunately, uncommon. We can differentiate between those tumors that are inside the brain (or intra-axial) and those that are inside the skull and compress the brain (extraaxial). Within intraaxial, the most frequent are gliomas, and within the extraaxial, the most frequent are meningiomas. We will mainly refer to these tumors to avoid being "encyclopedic".
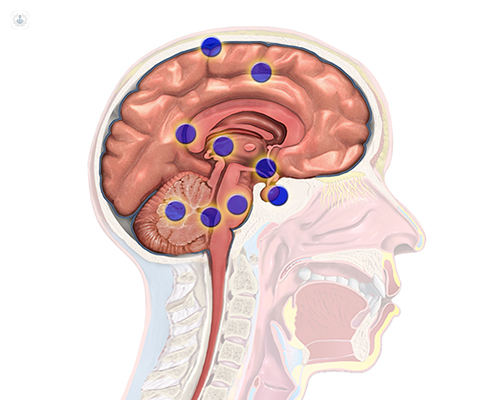
Brain metastases are even more frequent than gliomas and meningiomas, and we will treat them separately.
Intra-axial tumors
The most frequent of this type are the metastases of cancers originated outside the brain (breast, lung, etc.), but since they depend on an extracerebral disease they have a different treatment.
The most frequent intra-axial tumors are gliomas, tumors dependent on glia cells, which form the brain tissue next to and support neurons. These cells are called oligodendroctos and astrocytes, and tumors derived from them are oligodendrogliomas and astrocytomas, although there are also mixed tumors.
These glial tumors are in general diffuse, that is to say, although it seems that they are confined in a specific place we know that there may be tumor cells at a distance. They are usually characterized in 4 degrees: 1, 2, 3 and 4, according to their malignancy. 4 is the worst, and is called glioblastoma; Grades 2 and 3 are intermediate; Grade 1 is the only one that can be considered benign and the only one that can be nodular (not diffuse).
Treatment of intra-axial brain tumors
Its treatment is always based on surgery, directed either to make the greatest possible resection, or, in those cases in which the tumor is very widespread, to know exactly the nature of the tumor. It is very important to have a tumor sample, since until recently tumors were classified by their appearance under a microscope, the presence of molecular markers, which inform on the prognosis and optimize the treatment, is increasingly important.
In grade 1 and 2 tumors, if the resection is complete or nearly complete, sometimes it is not necessary to perform further treatments, although it will be kept under observation, performing magnetic resonances periodically. At other times, considered "high risk", will be proposed a treatment with radiotherapy or chemotherapy.

In grades 3 and 4, radiotherapy and chemotherapy are performed after surgery, even with complete resections.
The type of treatment will always be decided in a neurooncology committee, where the specialists involved (neuro-oncologists, neurosurgeons, neuroradiologists and neuropathologists) will take the best option in a consensual and individualized way.
Regarding the surgery of glial tumors (gliomas), the greatest possible resection should be performed, even greater than the tumor itself, ie a supra-septal resection, if this is possible. This is done by doing surgery with the patient awake, so that you can resect brain beyond the limits that the images gave to the tumor, safely for the patient. To perform this type of surgery, guided by the function and not by the image, it is necessary to collaborate with neuropsychologists, neuroanesthetists and, above all, the patient, since this success depends on the success of the surgery.
Role-guided surgery allows the removal of tumor cells that were distant from the area delimited by imaging techniques (magnetic resonance imaging) and decrease the possibility of tumor recurrence or regrowth.
It is also frequent for its usefulness the use of intraoperative techniques that allow delimiting the tumor by contrasting it and thus differentiate it from the surrounding brain tissue, such as the 5-ALA technique or fluorescein. These techniques allow the entire tumor to be resected, but they do not prevent the occurrence of secondary lesions.
Extraaxial tumors
The most frequent are meningiomas and neurinomas (schwannomas). They are tumors that do not originate from the brain, but from the adjacent tissues (meninges or nerves) and compress the brain. In general, they are benign tumors, although there are very aggressive variants of both tumors.
They tend to have a slow, but inexorable, growth, and if they are completely removed they can be cured, although this extirpation may be impossible because of the size they may have, because of their location or because they surround vital structures. Whenever possible, complete excision should be performed, although there are exceptions, such as very small tumors or multiple silent tumors, etc.. Another therapeutic possibility is radiosurgery, which consists of irradiating the tumor in a single session with very high doses of radiation. This technique allows to control the tumor, that is to say, to avoid its growth, reason why it is very useful in asymptomatic tumors (although it has a limitation of volume: it can only treat tumors of a diameter smaller than 3 cms.). However, it is not useful or advisable in tumors that cause symptoms by compression of the brain or nerve.
There are other types of irradiation, such as fractional stereotactic radiotherapy, which also applies to this type of tumor. It is similar to radiosurgery but is performed in several sessions and is reserved for tumors of greater volume or very close to radiosensitive structures, such as the optic nerve or the auditory apparatus.
It is possible, and indeed is increasingly advised, to reduce the size of tumors by surgery, leaving a rest that can be treated by radiosurgery, which allows to improve symptoms and decrease surgical risk.
Again, it is necessary that the neurosurgeon who evaluates the case has experience in microsurgery and radiosurgery, to be able to advise the best option, since in tumors of this type, it is essential to maintain the functionality, which is what allows to maintain a good quality of lifetime.