When benign prostatic hypertrophy appears?
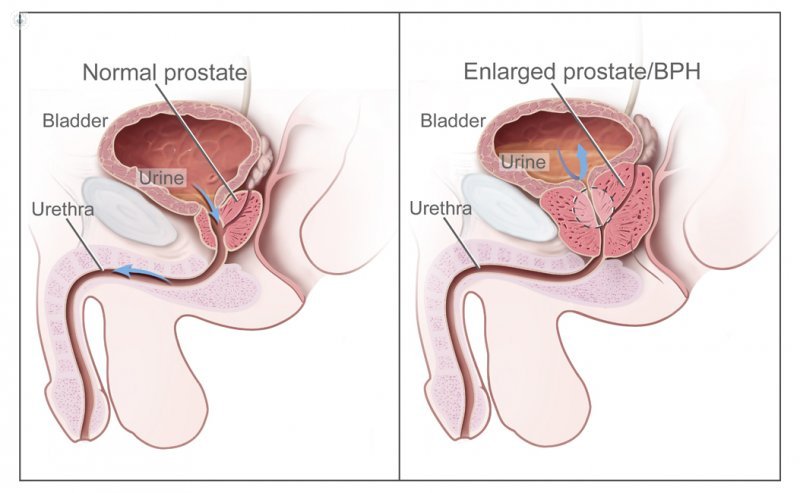
Written by:The prostate is an accessory sexual gland located on the underside of the bladder, posterior to the pubis and anterior to the rectum. From the age of 50, sometimes before, the prostate undergoes a benign growth known as benign hypertrophy.
Benign hypertrophy consists of hyperplasia of the fibromuscular and glandular tissue of the prostate.
Since there are no conclusive data to demonstrate what types of dietary habits or lifestyle can influence their appearance, there are currently no recommendations for avoiding prostatic hyperplasia.
Symptoms of benign prostatic hypertrophy
The set of symptoms of benign prostatic hypertrophy is known as prostatism. This concept encompasses both irritant and obstructive symptomatology.
The most common irritant symptomatology is:
- Frequent urination during the day (diurnal pollakiuria)
- Need to urinate during the night (nocturia)
- Imperative urges to urinate (urgency)
- Hypogastric discomfort
The most frequent obstructive symptomatology is:
- Delayed onset of urination
- Decrease in jet gauge and force
- Intermittent urination
- Urinary retention
- Overflow incontinence
Risk Factors for Benign Prostatic Hypertrophy
Although it may be earlier, benign prostatic hypertrophy usually occurs in men over 50. The symptoms usually develop in different ways in each patient, so it is difficult to know how it will evolve in each man.
There are indications that a man older than 60 years and with symptoms of prostatism is more likely to require prostate surgery in a period of 10 years than without symptoms.
Consequences of benign prostatic hypertrophy
According to specialists in urology , benign prostatic hypertrophy causes worsening in the patient's quality of life. The evolution over the years of benign prostatic growth can lead to chronic retention of urine in the bladder, to the formation of bladder stones, and even to urethral and renal dilatation, which can lead to kidney failure.
Treatments of benign prostatic hypertrophy
There is currently no consensus on the indication of treatment. The therapeutic possibilities are multiple and range from pharmacological treatment to traditional surgery, through multiple minimally invasive alternatives.
It is the urologist who has to assess which medical indication is most appropriate in the treatment of each patient.
When medical treatment fails or there are additional problems, the surgical treatment is summarized in transurethral resection with mono or bipolar energy, cervicotomy, prostatic vaporization, and adenomectomy with holmium laser or conventional surgery.
Depending on the prostate volume and the technology available to the urologist, any of these possibilities may be the ideal treatment for the patient.