
How to prevent sarcopenia, a disease for which there are no drugs yet
Written by:Prevention of sarcopenia should begin in adulthood , since loss of muscle mass and function begins around the age of thirty and becomes more prominent after the age of fifty. Prevention is based on maintaining a high level of physical activity in daily life, carrying out specific resistance exercise, adequate nutrition and avoiding risky behaviors (smoking, drinking alcohol). Establishing these habits may delay the onset of sarcopenia, possibly more than a decade, depending on the age at which the changes begin.
It is probably worthwhile to use screening tests to detect it in this population, although there is still no agreement as to which age to start looking for it, nor has it been shown that population screening improves relevant clinical outcomes.
An alternative is to look for sarcopenia in certain care settings or at risk populations. The largest admitted to hospitals, residences or rehabilitation centers, and those who visit Geriatrics are groups of special risk; Repeated falls, those who seem to walk more slowly, those who have a prolonged limitation of their physical activity, those who use a walking stick or crutch, or those who have trouble getting up from the chair.
Treatment of sarcopenia
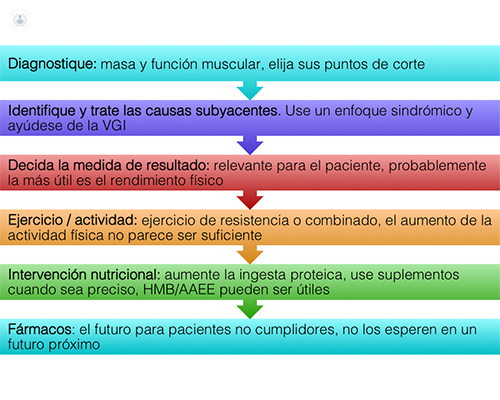
Treatment of sarcopenia should necessarily include resistance exercises and improved diet, increasing protein intake to 1.2-1.5 g / kg / day and covering the caloric requirement. In some cases, it will also be necessary to use nutritional supplements, which may contain leucine, HMB and vitamin D to optimize their effects on muscle.
It is also recommended a proportionate distribution of proteins throughout the day, emphasizing protein intake immediately after exercise, since the muscle seems to take priority at that time to receive the proteins ingested.
We still do not have drugs to treat sarcopenia.
Pathophysiology of sarcopenia
The pathophysiology of sarcopenia is very complex, including both muscle processes and endocrine and neurological regulatory processes.
With normal aging, the quality of muscle fibers deteriorates, reducing their maximum power, shortening speed and elasticity.
There are also anatomical changes, with a reduction in the number and activation of muscle satellite cells, a reduction in the number of muscle fibers (especially type IIA) and fat infiltration of muscle. The circulating levels of myostatin also increase with age and the regulation of various genes regulating muscle protein metabolism is modified.
On the other hand, the neurological control of the movement is also affected.

